
Challenge
How might we bridge the gap and facilitate open, non-judgmental conversations between young people and the providers who care for them?
Results
CoT created groundbreaking outcomes on consults tested. Young people felt listened and empowered to ask all kinds of questions.
Non-designers from Ci3 were impacted by the the human-centered design approach. This project was considered a turning point for the design team within the organization. The academic research center is applying for NIH grants to fund the implementation of CoT.
All medical providers, including pediatricians, OB/GYNs, psychiatrist among other, who were engaged in the research process were interested in taking the design intervention forward in their appointments. CoT will be officially launched in 2020.
design research, strategy, project management, prototyping, storytelling, modeling complexity, visual design
Cards On The Table
Building trusting relationships between providers and patients.
Project executed within the University of Chicago's Center for Interdisciplinary Inquiry and Innovation in Sexual and Reproductive Health (Ci3)







What is Ci3?
Ci3 is a faculty-led initiative to advance sexual and reproductive health, rights and justice locally, nationally, and globally. With a particular focus on adolescents, women, and communities of color, the goal is to develop new research methodologies, evidence, intervention strategies, and novel solutions to advance human health and well-being.
“There’s a disconnect between sexual and
reproductive healthcare — and young people.”
During the summer of 2019, I worked in the Design Thinking Lab at Ci3 with the concept "Cards On The Table" (CoT), generated as an idea for provider curricula. It was highly favored among young people and providers.
Sexual and Reproductive Healthcare — the gap between young people and providers
Literature and anecdotes tell us that young people do not feel comfortable raising topics about sexual health with a provider verbally. In the exam room, providers may intuitively sense that there is a question the young person wants to ask, but chooses not to.
“I feel iffy towards doctors because — I don’t know, it feels weird to me. I never know how they would tell me some type of information or if they would be judgmental about me asking questions. Or they might tell my parents about what I said.”
“We have an assumption that young people don’t have questions or want to ask providers about them if they do.”
Building enough rapport with a young person to have an open conversation about other sensitive topics in 15 minutes is not always a realistic scenario. Lastly, while intake forms can capture useful information for a provider, they are also challenging to change. Intake forms require approvals from many layers of the clinical institution, including legal. They are also often based on risk assessments, which can feel shaming for the patient completing them.
Design Intervention
“Card on the Table” started as a set of cards with sexual health topics on them. A young patient would pick these up at registration or in the exam room and select topics that they would want answered during their consultation. When the healthcare provider enters the room, the provider would ask them what questions they are interested in.


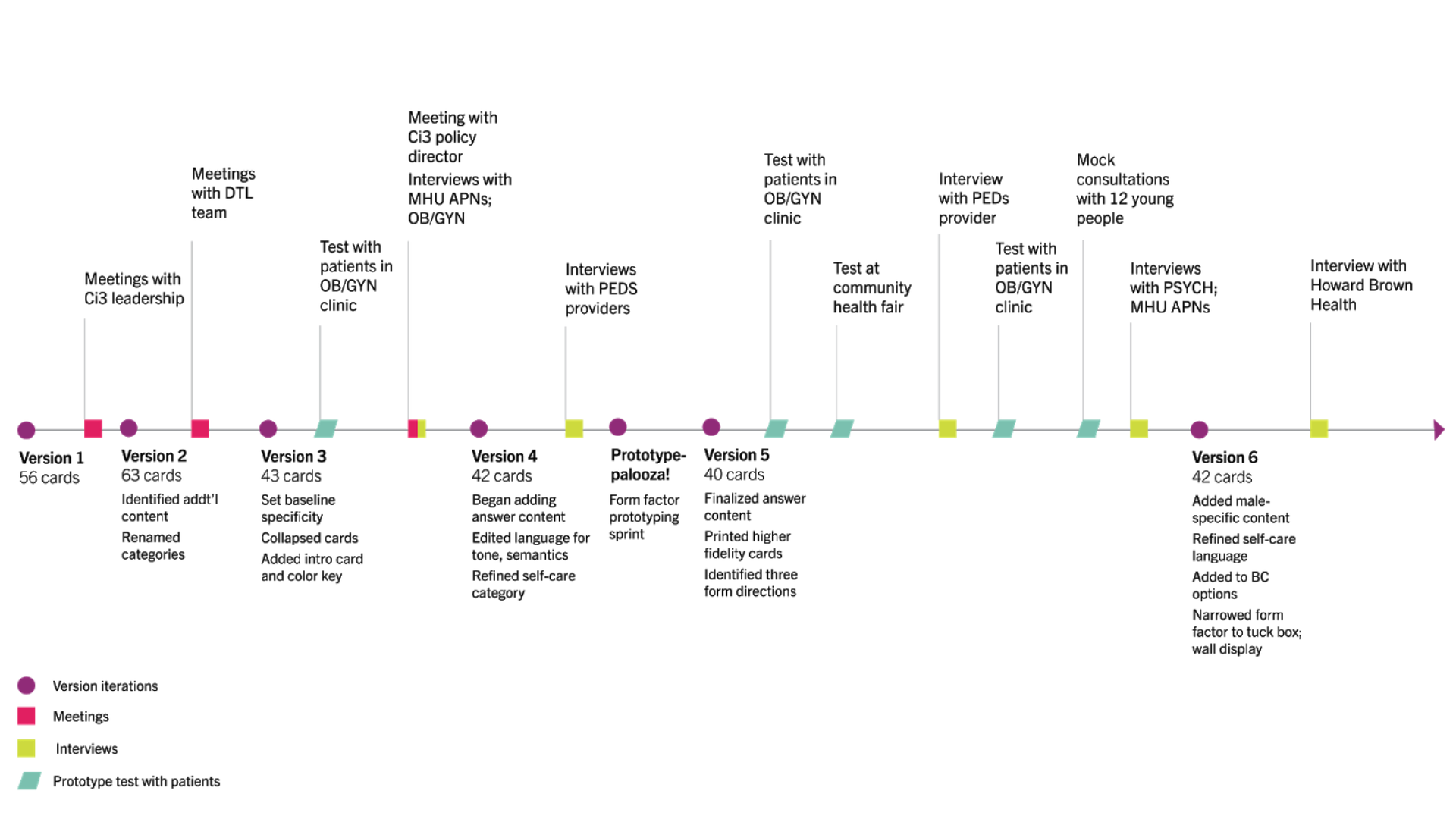
Research
We conducted more than 40 interviews and prototype testing sessions with different kinds of providers (Pediatricians, OB/GYNs, Psychologists, APNs, medical assistants, social workers, among others) and patients (in clinic and mock consultations). The project was driven by rigorous PARTICIPATORY DESIGN methods. See below for more details about the design process timeline.

During research we addressed questions of content and form. Here are a few of the questions explored:
1/ What selection of content will speak to young people’s most common SRH concerns, while embracing a wide range of topics?
2/ How can we balance using language that resonates with young people and medically accurate terminology?
3/ Is there an ideal number of cards? How many is too many? Or too few?
4/ What different ways might young people use CoT? Can it both support existing questions and provoke new ones?
5/ What age groups and contexts of use is CoT appropriate for?
6/ What advantages does CoT offer providers? Why is it beneficial rather than a burden?
Designing Cards on the Table
It was critical going into the clinic setting with designed pieces for interviewees—clinicians, patients, and family members—to get their reaction to it on the spot. As such, we developed early “provotypes” based on hypotheses generated from our literature review and initial conversations with clinicians and patients. These were then iterated upon over the span of several weeks.


Form Exploration
In order to get the CoT goals delivered to best optimize open and non-judgemental conversations between young patients and providers, different form factors were developed to address the gap among stakeholders. Bearing in mind the clinic flow, privacy, production cost, information structure, approachability, etc, we designed 3 forms of the concept.
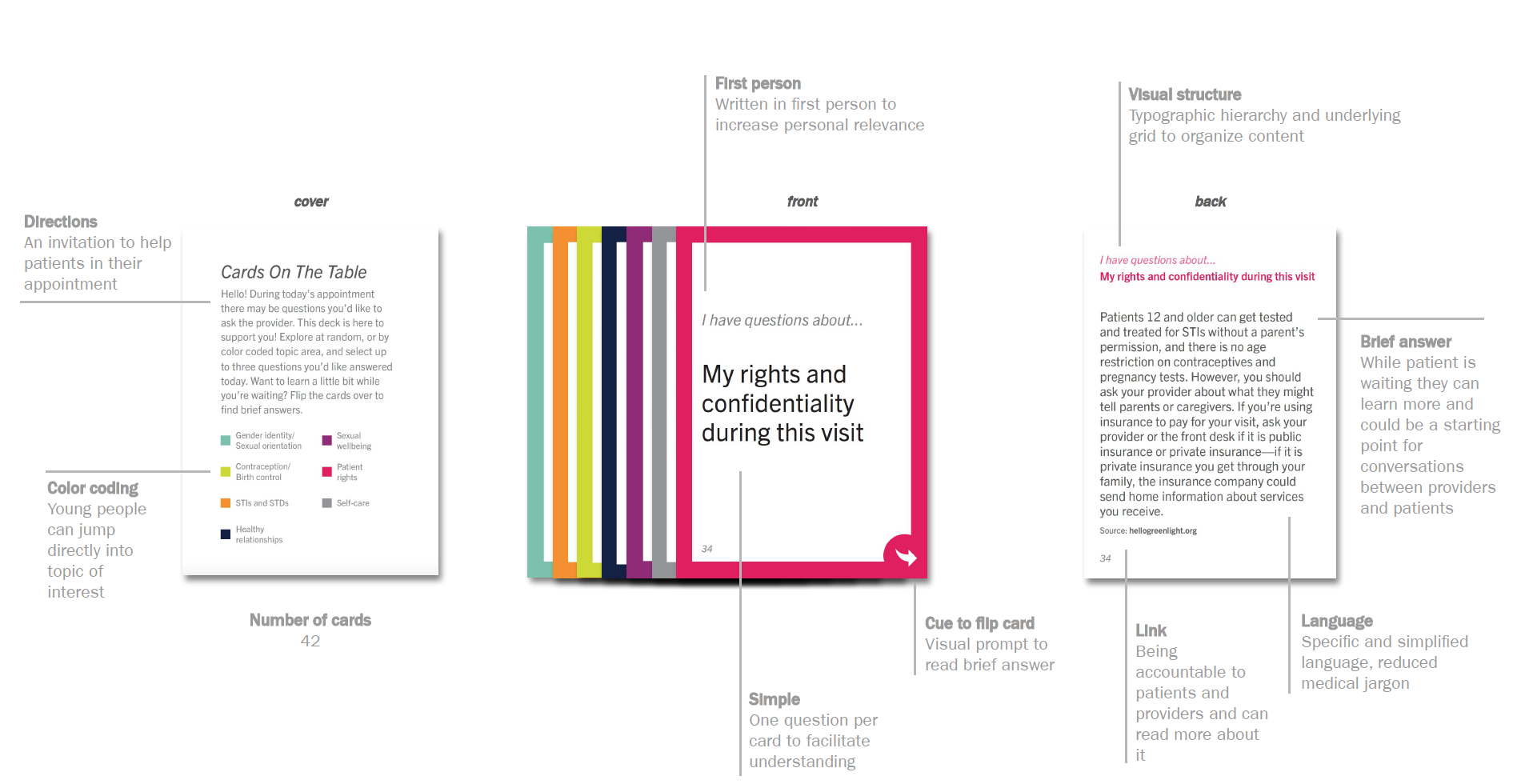
Anatomy of a Card
The refined high fidelity prototype includes several key advances in design to improve communication of ASRH between patients and providers, empowering young people and revealing as a key for quality of care.
Possible Clinic Flows
CoT was designed in a way that would be flexible enough to be used in different contexts and clinic flows.

Learnings
1/ Normalizing v.s. reinforcing stigma: Natural tension emerged between normalizing and reinforcing stigma about SRH topics, particularly when we considered how how visible/discreet to make the intervention.
2/ Disrupting a mental model: The passive presence of a tool encouraging SRH conversations can help expand mental models about where SRH care belongs.
3/ Increasing effectiveness: While CoT is flexible enough to be delivered in any clinic flow, it seems to be particularly effective when coupled with an open and conversational approach from the provider.
Further Exploration
1/ Develop a strong point of view for content on the backs of cards: workshop with multiple stakeholders, parent and young people focus groups.
2/ Prototype and test a “how to use” guide for providers
3/ Identify and source ideal materials
4/ Spanish translation with parents and young people
5/ Explore alternative contexts of use: sex ed tool for schools; conversation starter with adults; inpatient use.
6/ Test all form factors in different settings: in mobile health units, school-based health clinics and PEDS clinic.
SPECIAL THANKS TO THE WHOLE TEAM
Co-leads: Julia Rochlin and McKinley Sherrod
Ci3 / DTL Team: Amanda Geppert, Emily Moss, Sierra Ribero, and all our colleagues at Ci3.
Institute of Design Faculty/Advisor: Ruth Schmidt